




















Growth and Tolerance with an Amino Acid Based Enteral Formula: A Two-year Retrospective Study from a Children's Rehabilitation Hospital
Hulsey A, Cekola P, Henrikson A, Reichert H, Cohen SS, et al. (2022). J Clin Nutr Diet Vol.8 No.8:181.
Introduction:
For medically complex children, optimal care including well-tolerated nutrition that is complete and balanced is key to growth, development and quality of life. Use of amino acid-based formulations has been recommended for some infants and children with medically complex conditions that affect nutrient absorption and utilization, i.e., conditions of genetic, metabolic, and neurologic origin. This study was a retrospective assessment of children who were switched to a specialized hypoallergenic, amino acid-based formula while staying at a children's rehabilitation hospital. The study population included children >12 months who had medically complex conditions and needed enteral tube feeding. The primary aim of this study was to describe the population of medically complex children fed AA-MCT.
Methods:
This study was a retrospective review of medical records of pediatric patients who stayed in a children’s hospital rehabilitation center and were switched to the AA-MCT formula. Demographic data were compiled, and outcomes data (nutritional status, feeding tolerance, GI medication use, growth) were collected at five time points over two years (12 months pre-switch to AA-MCT formula, 6 months pre-switch, at switch, and at 6 and 12 months post-switch). The intervention was a nutritionally complete formula (Alfamino® Junior, unflavored, Nestlé Healthcare Nutrition) that was free amino acid-based (AA) with medium-chain triglycerides (MCT).
OUTCOME MEASURES: The primary objective of this retrospective study was to describe characteristics of the population using the AA-MCT formula, including subject demographics (age, sex, ethnicity); primary and secondary diagnoses and medical conditions that were indications for use of the AA-MCT formula. Secondary outcomes were growth (weight and height), achievement of nutritional goals (average intake of formula consumed over 7 days, at each time point), feeding tolerance (vomiting, flatulence, stool frequency and consistency), and GI medication use (proton pump inhibitor, H2 blocker, prokinetic agent, anti-diarrheal, fiber supplement, laxatives, stool softeners, antiemetic, other). These measures were compiled for time points 12 and 6 months prior to transition to AA-MCT formula, at the time of the formula transition and then assessed again at 6 and 12 months while AA-MCT formula intake continued.
Results:
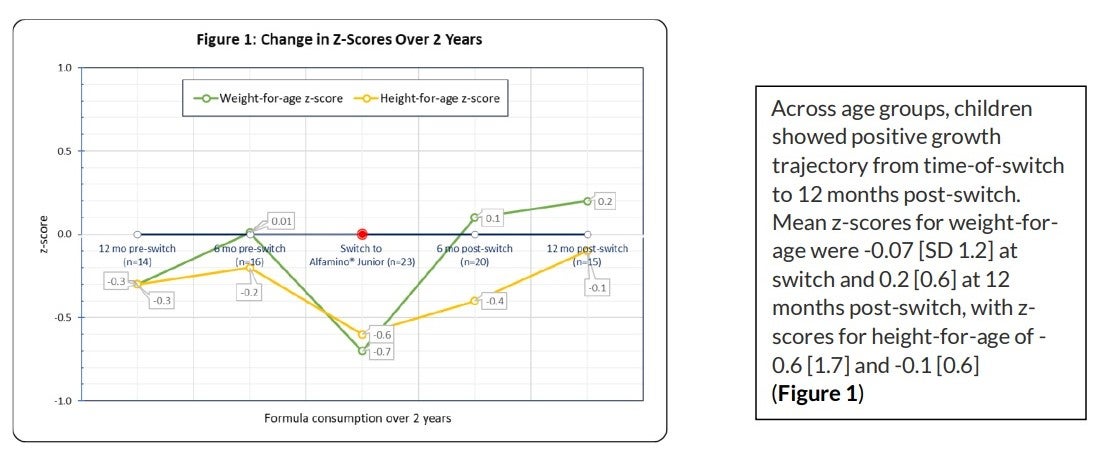
The medical records of 26 children, aged 1 to 18 years, were identified, and reviewed; 3 subjects were excluded due to insufficient data, leaving 23 subjects. At initiation of the AA-MCT formula, the mean age of the children was 7.5 ± 5.4 years, 61% were female, multiple ethnicities were represented (48% Caucasian, 35% African American, 13% American Indian/Alaska native, 4% Asian), and 100% were tube fed (70% via gastrostomy, 30% via gastrojejunostomy tube). A variety of primary diagnoses were observed; 48% presented with a GI disorder, which included atrophic gastritis, delayed gastric motility, diarrhea, flatulence, gastroschisis and vomiting. Other primary disorders (17%) included: DiGeorge syndrome, chronic transaminitis, failure to thrive and other metabolic diseases/disorders. Feeding disorders and atopic dermatitis each accounted for 13%, respectively. Allergies to milk, soy, wheat, peanuts, egg, and red dye were present in 9% of the population. Prior to switching to AA-MCT, enteral formula use varied; the most common formula children received was another amino acid formula (for children aged 1+ year), followed by standard pediatric formulas, and then extensively hydrolyzed formulas. In the year prior to the switch to the AA-MCT, lower calorie/protein prescription and intake was noted in 60% of the children. Upon switching to the AA-MCT, intake for calories and protein increased for all children, and the increases were sustained in most of the children (n=20) at 6 months post-switch. Overall, intake of calorie and protein goals was achieved. The mean percentage of daily intake at switch to AA-MCT was 100% for calories and 99% for protein. At one-year post-switch, 99% of calorie and 99% of protein goals were maintained. Overall, adequate growth was achieved, evidenced by appropriate increases in weight-for-age and height-for-age at both 6 and 12 months post-switch for both boys and girls across all age groups. Similarly, height-for-age mean percentiles were 47% and 51% (CP growth charts, N=18); 23%, and 9% (WHO growth charts, N=5, N=1, respectively). Weight-for-age mean percentiles at switch and 12 months post-switch were 57% and 60%, respectively, for children on CP Growth Charts (N=18) and were 28% and 33% for children on WHO Growth Charts (n=5).
TOLERANCE & GI MEDICATION USE: Over time there were no significant changes in GI tolerance events. Upon switching, the AA-MCT was generally well tolerated. There were no reports of formula discontinuation post-switch. The number of stools per child per day were a mean of 2.1 [SD 1.1] at switch as compared to 1.6 [1.1] stools per day at 6 months prior to initiation of the AA-MCT formulation. Stools per day decreased to 1.5 [0.9] at 6 months post-switch and 1.6 [1.2] at 12 months post-switch, with consistently soft stool consistency. Throughout the 2-year review, the mean number of GI medications per subject, ranged from 1.6 to 2.6. At switch to AA-MCT, the children (n=23) received a mean of 2.3 [1.2] GI medications. The most frequent GI medications prescribed were laxatives (40%), proton pump inhibitors (15%), antiemetics (15%), H2 blockers (11%), prokinetic agents (6%), and stool softeners (4%). At 1 year post formula switch, 25% (4 of 16) of children were prescribed an additional medication, 44% had no change in GI medications, and 31% had a reduction in 1 or more GI medications.
Conclusions:
Our study findings showed that children aged 1 to 18 years with a variety of clinical diagnoses could benefit from a switch to a specialized formula containing readily absorbable amino acids and medium-chain triglycerides. Our study population exhibited good feeding tolerance and growth, as evidenced by meeting nutritional and growth goals up to 1-year post-switch. We observed age-appropriate growth for children with a wide range of immunologic, genetic, metabolic, neurologic, and developmental conditions associated with malabsorption and some children observed a reduction in GI medications after switching to AA-MCT. Such findings indicate that specialized nutrition for medically complex children can contribute to optimal care.
Download PDF of Summary. The study can be accessed here:Growth and Tolerance with an Amino Acid Based Enteral Formula: A Two-year Retrospective Study from a Children's Rehabilitation Hospital | Insight Medical Publishing (imedpub.com)
Study Summary Prepared by Nestlé Health Science. All trademarks are owned by Société des Produits Nestlé S.A., Vevey, Switzerland. ©2022 Nestlé. All rights reserved.