




















A Randomized Controlled Trial Assessing Growth of Infants Fed a 100% Whey Extensively Hydrolyzed Formula Compared with a Casein-Based Extensively Hydrolyzed Formula
Fields D, et al.
Global Pediatric Health. 2016. Volume 3: 1–9.
Objectives:
The study evaluated the effects of 100% whey protein, extensively hydrolyzed formula on overall growth and tolerance in healthy, term infants by comparing weight gain in healthy infants with a group of infants receiving a similar commercial formula from 2 weeks to 4 months of age. Additional measures included length and head circumference (HC), feeding tolerance, serum albumin and plasma amino acids.
Background:
Approximately 2% to 3% of infants are allergic or intolerant to cow’s milk protein formula and require a hypoallergenic formula. The American Academy of Pediatrics (AAP) recommends extensively hydrolyzed formula (EHF) for the dietary management of infants who are allergic or intolerant to intact cow’s milk formula. Hypoallergenic, 100% whey, extensively hydrolyzed, nutritionally complete infant formula designed for the dietary management of infants with cow’s milk protein allergy (CMPA) has been developed with the additional ingredients of probiotic, B.lactis and medium chain triglycerides (MCTs).
Statistical Methods:
The primary objective of this clinical trial was to assess growth (weight gain in grams per day) in infants fed the test formula (Extensive HA®) compared with those fed the control formula (Pregestimil). 56 infants completed the study in each group.
Methods:
A randomized, controlled, double-blind, multicenter clinical trial of 2 formula groups (Extensive HA® by Nestle with B.lactis and MCT or Pregestimil® with MCT by Mead Johnson) in parallel conducted at 25 sites throughout the United States. Infant participants were healthy, full-term (>37 weeks gestation), exclusively formula-fed infants with birth weights ranging from 2500 to 4500 g, whose caregivers had given informed consent to participate in the study, Infants received the formula for 112 days of life. Study visits were scheduled at 14, 28, 56, 84, and 112 days of life, where weight, length, and HC were measured. Caregivers kept a detailed record of formula intake, stool characteristics, spit-up, vomit, sleep, and mood.
Results:
Caregivers of 282 infants consented to their infants participating in the study, and were randomized to control (Pregestimil®, n=158) or test Extensive HA®, (n=124). The control group had significantly higher overall drop-out rate than the test group with a significantly higher number of drop-outs caused by adverse events (AEs) and loss to follow up. Birth weight, length, and HC were similar between the groups. In the PP population, no statistical differences existed except in boys at 112 days of age for absolute weight and weight-for-age percentiles and for boys and sexes combined at 84 and 112 days of age in z-scores, where the test group had greater weights for boys and sexes combined. In general, the control group had more frequent stools. The control group experienced more vomiting (13%) than those on test formula (7%) in the ITT population; Infants assigned to test formula had significantly (P < .001) fewer AEs than infants assigned to control formula.
Discussion
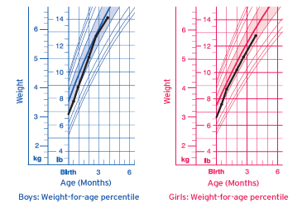
The weight gain observed in both groups was within the expected range of typical growth in infants of this age. Mean daily weight gains from 14 to 112 days were 27.95 g/d in the test group and 25.93 g/d for the control group. This difference between the 2 groups fell within the AAP-CON recommended difference of 3 g/d. For the purpose of the original intent of the study, noninferiority was demonstrated in terms of growth for the test formula. Although not evaluated, perhaps differences in actual stool volume could have affected weights. Participants in the control group did have significantly more stools. Although not evaluated, perhaps differences in actual stool volume could have affected weights.
Conclusion:
This multicenter 4-month trial demonstrated adequate growth in infants fed 100% whey-based EHF.
Demonstrated Growth & Tolerance:
Extensive HA® is a complete source of nutrition, clinically shown to promote adequate growth.
- Healthy, full-term infants, exclusively fed Extensive HA® from ~14 days of age demonstrated adequate growth after 4 months.
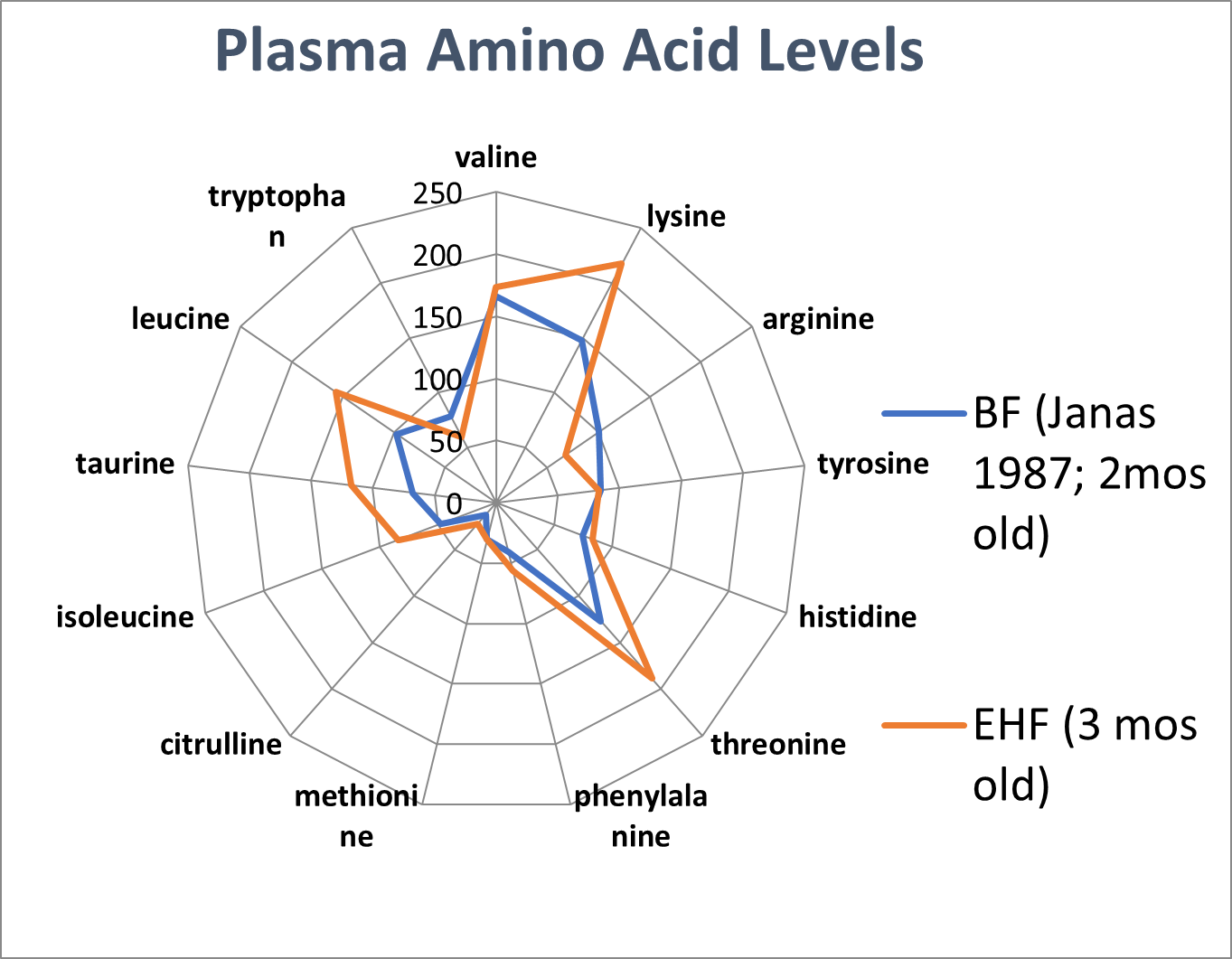
Extensive HA® delivered a plasma amino acid profile similar to breastfed infants.
- Plasma amino acid was similar in 3 months old infants fed Extensive HA®, compared to 2-month-old breastfed infants from a separate clinical trial (Janas et al. 1987)
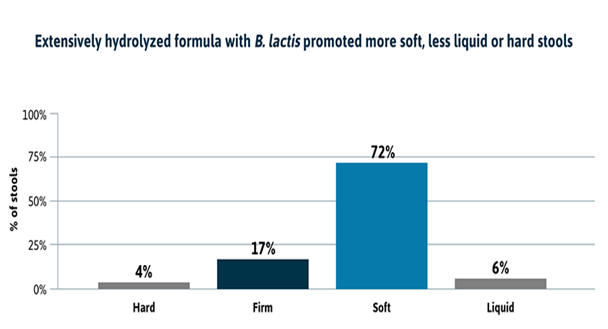
Extensive HA® promotes digestive tolerance & soft stools
- Infants fed Extensive HA® had soft stools more often than hard or liquid stools, and 0 infants developed diaper rash due to Extensive HA® (data on file 2016).
Study summary prepared by Nestlé Healthcare Nutrition.Download PDF of Summary
Link to publication: A Randomized Controlled Trial Assessing Growth of Infants Fed a 100% Whey Extensively Hydrolyzed Formula Compared With a Casein-Based Extensively Hydrolyzed Formula - PMC (nih.gov)
Pregestimil is a registered trademark of Mead Johnson & Company, LLC. Unless otherwise indicated, all trademarks are owned by Société des Produits Nestlé S.A., Vevey, Switzerland. ©2024 Nestlé. All rights reserved. Bridgewater, NJ 08807 U.S.A.