



















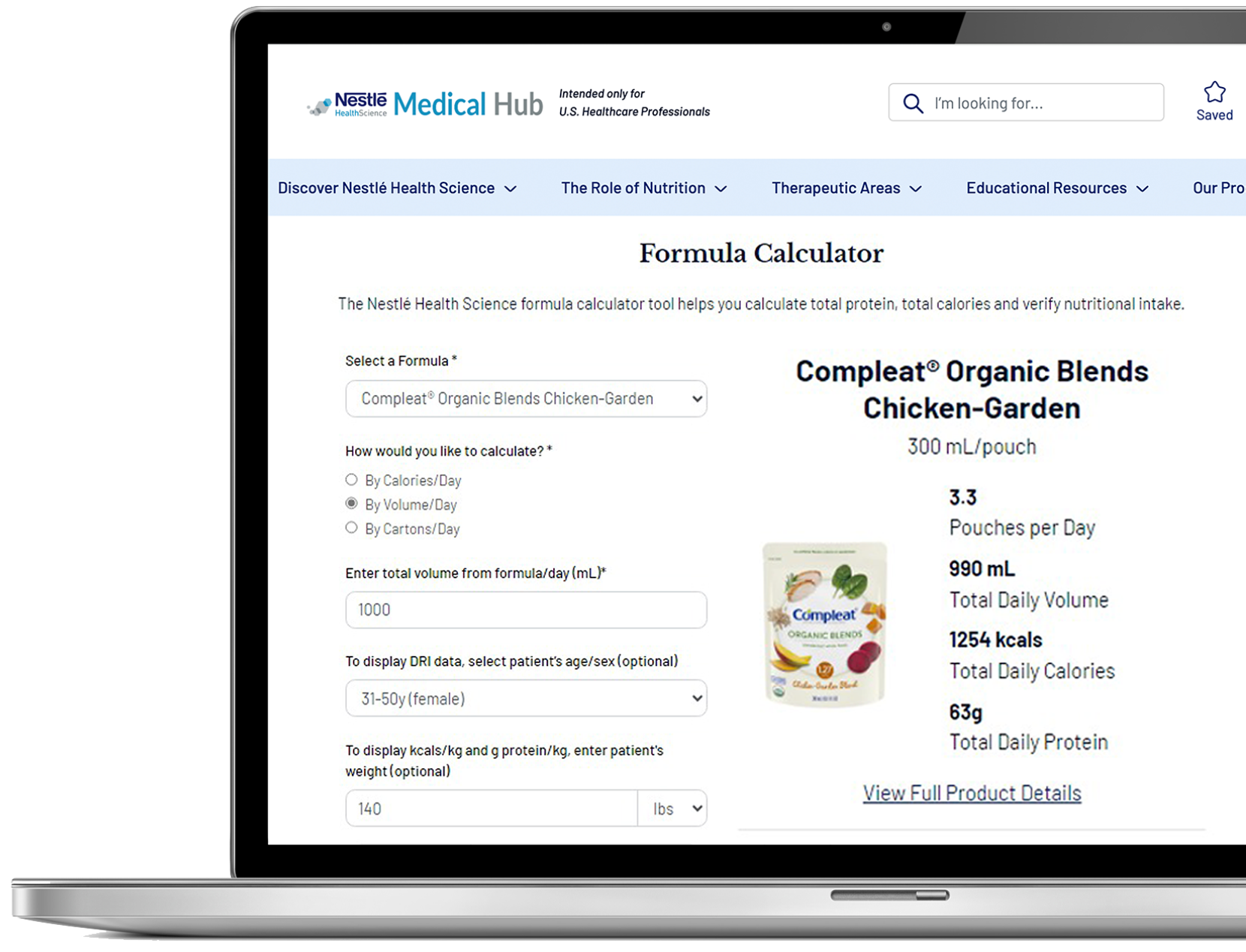

Progressive increase in protein delivery is associated with a significant improvement in mortality1
In a retrospective analysis of 2,000 ICU patient encounters, patients who received Peptamen® Intense VHP formula received significantly more protein at day 7 than when other enteral nutrition formulas were used (p<0.0001).1 A significant difference in 30-day mortality was shown in the group that received the very high protein formula (p=0.0001).1
Safety of Increasing Protein Delivery with an Enteral Nutrition Formula Containing Very High Protein (VHP) and Lower Carbohydrate Concentrations Compared to Conventional Standard (SF) and High Protein (HP) Formulas
Ochoa Gautier JB*, Berger A, Hussein R, Huhmann MB**. Clinical Nutrition. 2022;41:2833–2842.
Background
Conventionally, nutrition support of the critically ill patient has been focused on delivering adequate calories to prevent caloric deficit and the development of disease-related malnutrition. Many recent studies have failed to demonstrate the benefit of meeting protein and calorie goals during the first week of intensive care unit (ICU) stay. Recommended calorie amounts, timing of delivery and quality/amount of protein provided remains under investigation.
Objective
The purpose of this study was to determine the safety and clinical outcomes associated with the early use of a very high protein (VHP), lower carbohydrate (CHO) enteral feeding (EN) in the ICU.
Materials and Methods
- Retrospective analysis of existing electronic medical records (EMR) of adult patients admitted to the intensive care units (ICUs) in the Geisinger health care system who received at least 1 day of EN.
- Demographic and clinical data from the EMR included age, gender, admitting diagnosis, BMI, length of stay (LOS), readmission rates, in-hospital mortality, 30-day mortality and mortality upon readmission.
- All forms of nutrition delivery for first 7 days of ICU stay captured: estimated nutrition needs, enteral prescription, and total calories and protein delivered from all nutrition sources.
- Patients receiving exclusive oral or parenteral nutrition were excluded.
- Logistic regression analysis was used to determine correlation between protein delivered and clinical outcomes.
- EN Formula categorized into 3 possible groups:
- Standard/Low Protein: ≤20% calories from protein
- High Protein: 21–25% calories from protein
- Very High Protein: 37% of calories from protein; 29% calories from CHO
Results
- 2,000 medical encounters with 12,321 ICU days collected and analyzed.
- Most frequently encountered diagnoses included sepsis/septic shock/shock, cerebrovascular disease and other neurological conditions, acute or chronic respiratory illness, cardiovascular disease.
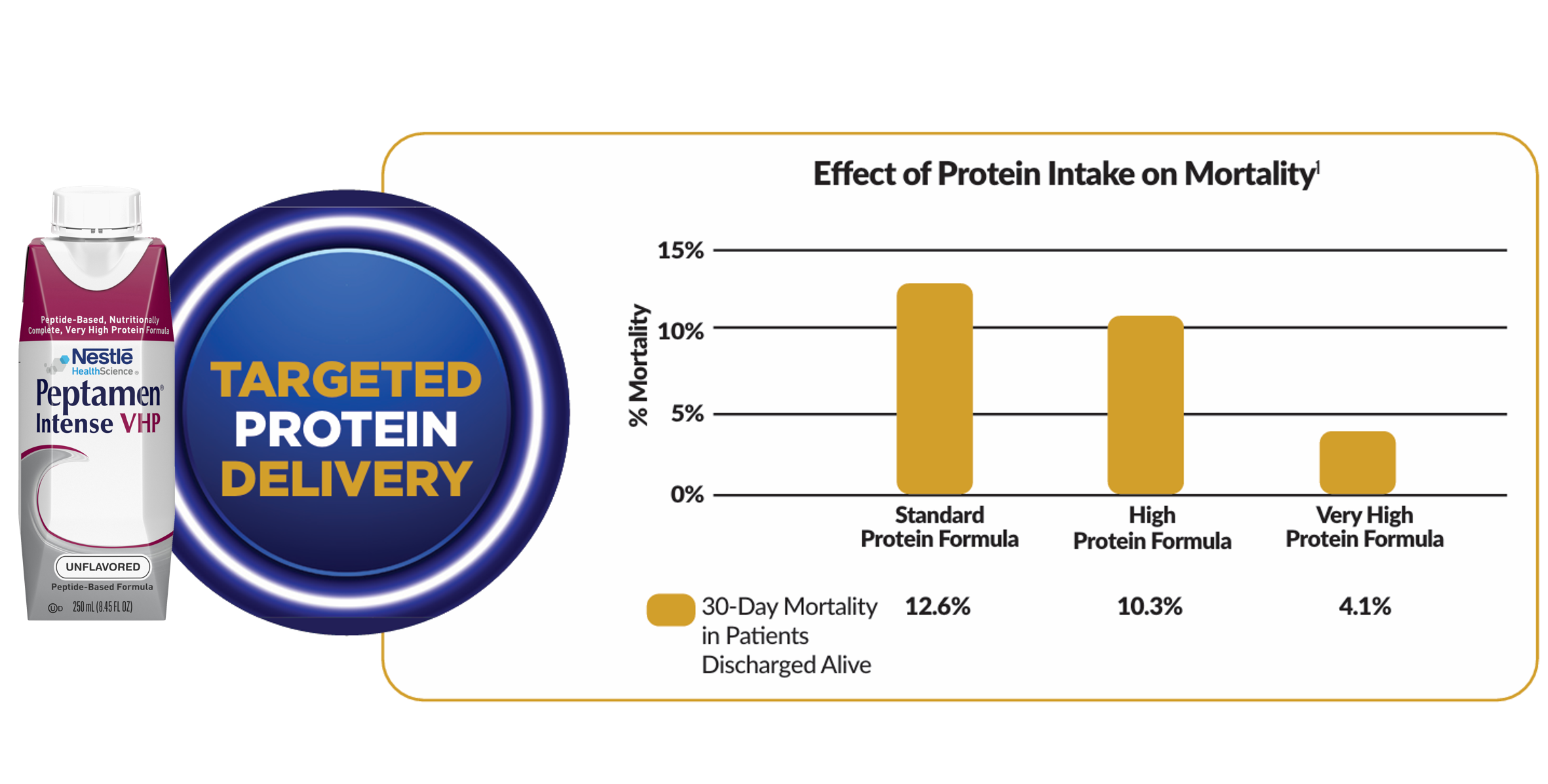
- Overall mortality during hospitalization was 7.5%; 30-day mortality among patients discharged alive was 10.6% (p=0.0004).
- Median hospital LOS was 13.6 days; ICU LOS was 6.9 days; invasive mechanical ventilation 4 days.
- 30-day readmission rate among patients discharged alive was 19.3%.
- Significant differences in 30-day post discharge mortality were observed by type of formula consumed, with mortality decreasing as the protein composition increased (p=0.0013).
- A composite of inpatient mortality and 30-day post-discharge mortality were significantly different between groups (p=0.0035) with a progressive decrease in mortality correlating with increasing protein concentrations in the EN formula used (p=0.0001).
Discussion
Catabolism and muscle loss is rampant in the critically ill. Early provision of full calories generally fails to spare muscle or achieve protein anabolism during the first week of ICU stay. Multiple randomized controlled trials have failed to show clinical benefit of providing full caloric support in the ICU. Critical care nutrition is currently in a paradigm crisis, forcing clinicians to reassess what and how much nutrition to deliver to patients. A gradual increase in protein over time with a goal of 1.3 g/kg/day by day 7 is suggested by some guidelines. The delivery of higher amounts of protein and lower amounts of calories is particularly challenging with conventional formulas where the calorie to protein ratios risk an excessive delivery of calories while providing limited amounts of protein. In addition, providing lower CHO feedings with high protein delivery improves glycemic/metabolic control. This study demonstrates that providing a VHP, lower CHO formula during the first 7 days of ICU stay is safe and may have a beneficial effect on 30-day mortality. Effect on muscle mass was not studied.
- A significant improvement in mortality is observed with gradually increased protein delivery and decreased CHO loads
- High protein, along with lower CHO intake appears to generate the best outcomes for critically ill patients
- Prospective randomized trials are warranted to establish causality