
Compleat® Pediatric Original 1.0 made with real food ingredients was well-tolerated and resulted in positive growth outcomes in two ex-premature, medically complex children

A retrospective, observational case series of two ex-premature children with medical complexity, gastrointestinal (GI) symptoms, and developmental delay transitioning from post-discharge infant formulas to Compleat® Pediatric Original 1.0 made with real food ingredients demonstrated GI tolerance as well as positive growth outcomes.
Nutritionally Complete Tube-Feeding Formula with Real Food Ingredients – Tolerance and Growth Outcomes in Ex-Premature Medically Complex Children
A Research Summary based on: Poster #P168 at ASPEN26 Nutrition Science and Practice Conference, February 14–17, 2026, Long Beach, California.
Minor GJ, Blackmer A. J Parenter Enteral Nutr. 2026; 50: S71–S332.
Why Was This Study Done?
- Providing optimal nutrition to ex-premature children with medical complexity and developmental delay (DD) can be challenging due to variable enteral formula (EF) tolerance and efficacy.
- Multiple EF trials may be required before finding a well-tolerated option, which may impact growth and development.
- Real food ingredient EFs offer benefits such as diversity of ingredients and fiber sources, positive microbiome effects and impact on digestive health, and immune support.
- Limited data exist related to a) specific pediatric populations that may benefit from real food ingredient EF, and b) growth outcomes using standardized evaluation methods (i.e., z-scores).
This study presents two ex-premature children with medical complexity, gastrointestinal (GI) symptoms, and DD transitioning from post-discharge infant formulas to a 1.0 kcal/mL pediatric tube-feeding formula made with real food ingredients (e.g., chicken, tomatoes, peaches, green beans, carrots, peas; Compleat® Pediatric Original 1.0, Nestlé Health Science, New Jersey [RFF]).
Patients
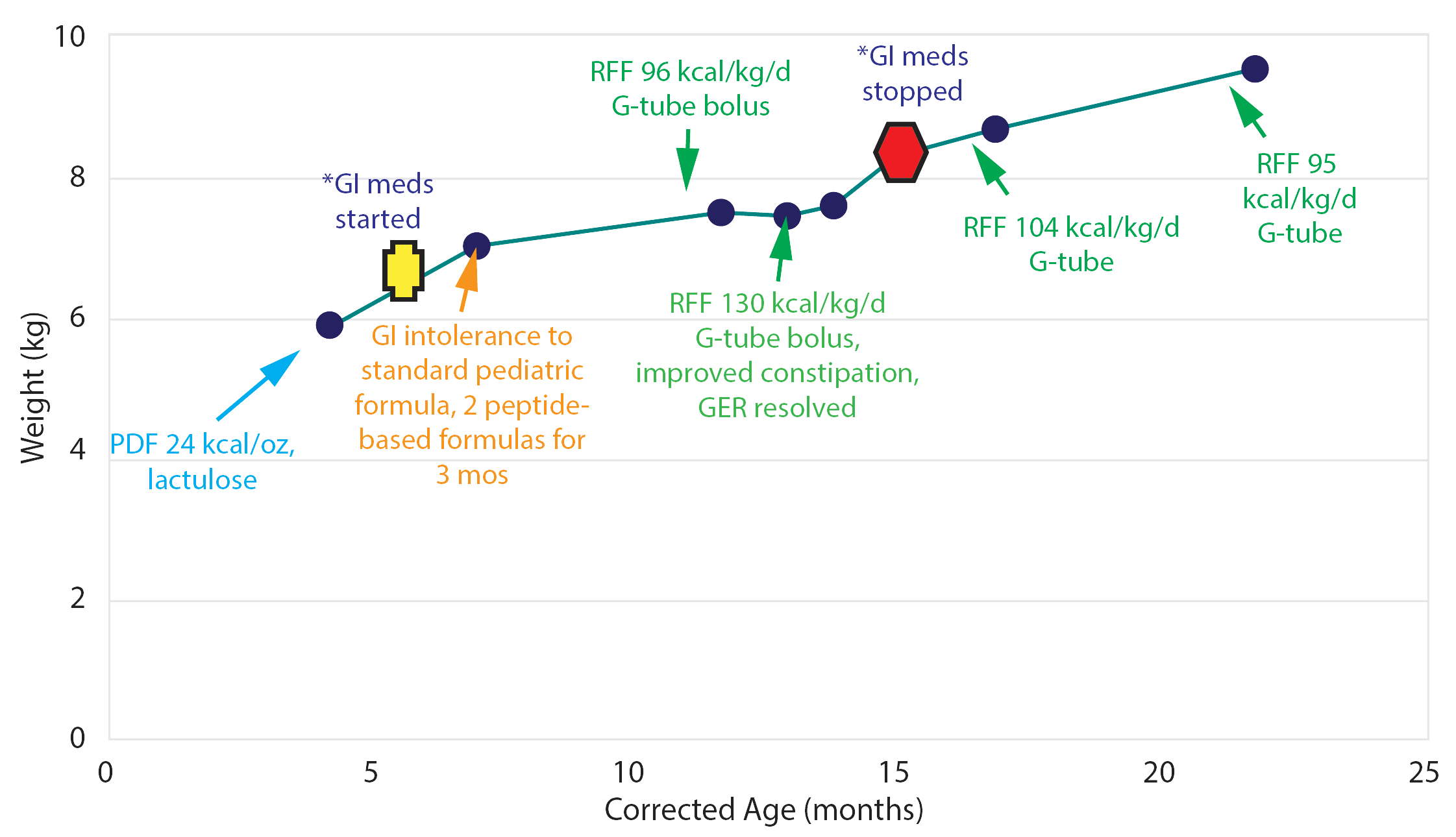
- Hospital discharge at 29 weeks (12 weeks corrected age) on 24 kcal/oz post-discharge formula (PDF) plus lactulose for constipation
- At 13 months (9 months corrected age), transition to pediatric EF attempted for 3 months: multiple EFs tried, resulting in intolerance, medication initiation (famotidine, azithromycin, metoclopramide), and lack of adequate growth
- RFF initiated at 97 kcal/kg/day via G-tube, leading to improvement of GI symptoms and initial improvement of growth (e.g., weight, height)
- RFF increased to 130 kcal/kg/day, resulting in continued clinical improvement, growth (e.g., weight, height, growth velocity) and medication discontinuation
- Hospital discharge at 34 weeks (19 weeks corrected age) on 26 kcal/oz PDF plus metoclopramide and esomeprazole for emesis and reflux — caloric density decreased (24 kcal/oz)
- At 13 months (9 months corrected age), transition to RFF at 106 kcal/kg/day via G-tube
- In first 3.5 months after switching, consumed purees and other foods for comfort plus RFF (106–117 kcal/kg/day) with adequate GI tolerance
- At 17 months (13 months corrected age), patient underwent ASD closure via median sternotomy
- By 19 months (16 months corrected age), reflux resolved, GI medications stepped down and sustained weight gain observed through 2 years of age
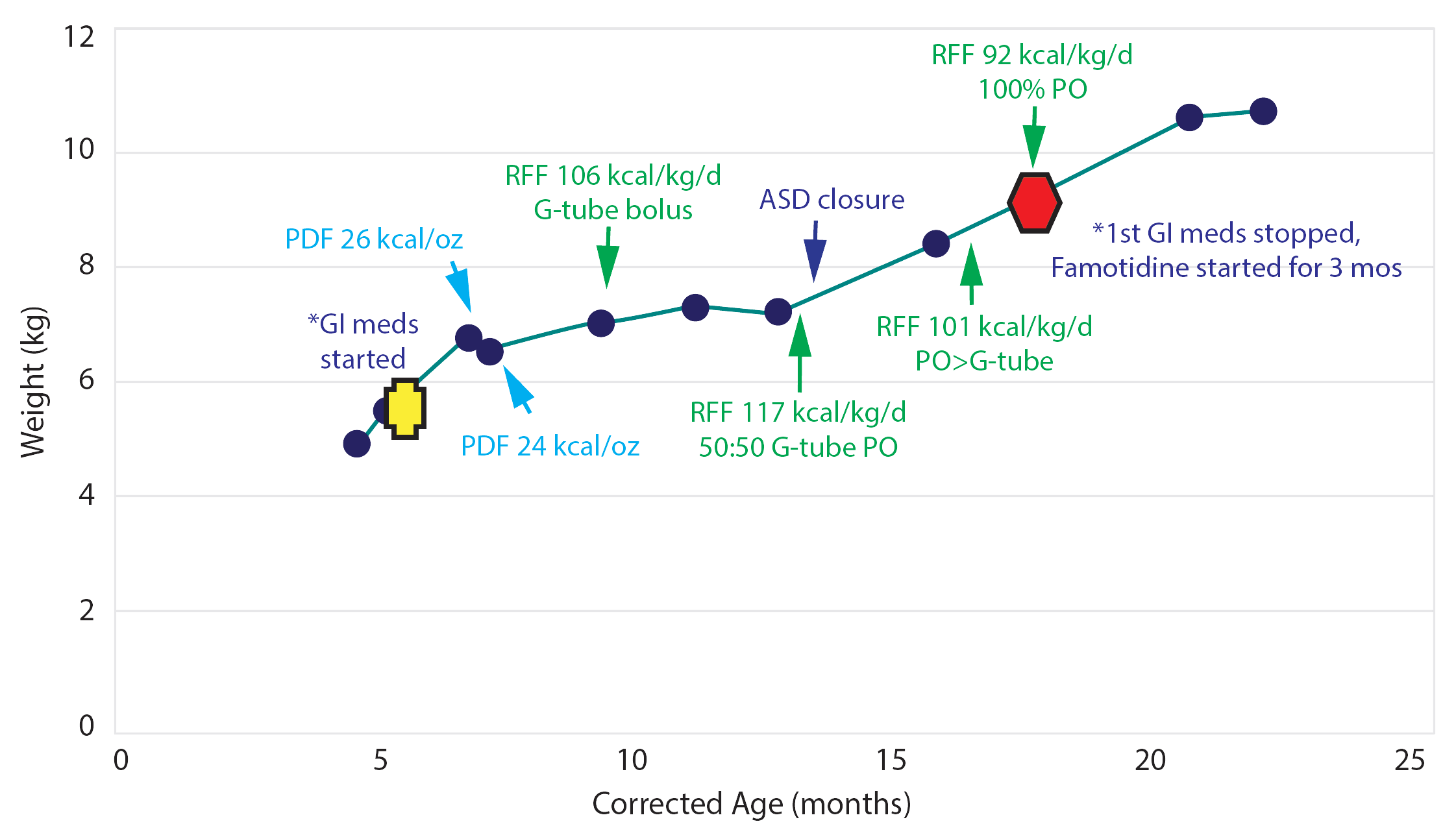
Abbreviations: PDF, post-discharge formula; GER, gastroesophageal reflux; GI, gastrointestinal; mos, months; RFF, pediatric tube feeding formula made with real food ingredients; ASD, atrial septal defect; PO, per os; DD, developmental delay; BPD, bronchopulmonary dysplasia; FD, feeding disorder.
- These cases provide real-world evidence of successful use of RFF in ex-premature children with medical complexity and significant GI symptoms transitioning from infant to pediatric enteral formulas, highlighting the benefits of real food ingredients in this population.
- While challenges can still be presented, these children demonstrated positive growth outcomes and RFF tolerance, evidenced by the ability to discontinue GI medications, highlighting the benefits of RFF in this population.