




















Safety of Increasing Protein Delivery with an Enteral Nutrition Formula Containing Very High Protein (VHP) and Lower Carbohydrate Concentrations Compared to Conventional Standard (SF) and High Protein (HP) Formulas
Ochoa Gautier JB*, Berger A, Hussein R, Huhmann MB** Clinical Nutrition 2022;41:2833-2842
Background:
Conventionally, nutrition support of the critically ill patient has been focused on delivering adequate calories to prevent caloric deficit and the development of disease-related malnutrition. Many recent studies have failed to demonstrate the benefit of meeting protein and calorie goals during the first week of intensive care unit (ICU) stay. Recommended calorie amounts, timing of delivery and quality/ amount of protein provided remains under investigation.
Objective:
The purpose of this study was to determine the safety and clinical outcomes associated with the early use of a very high protein (VHP), lower carbohydrate (CHO) enteral feeding (EN) in the ICU.
Materials and Methods:
This was a retrospective analysis of adult (≥ 18 years) ICU patients admitted to the Geisinger health care system from July 2012 – June 2015. Each patient admission to the ICU was considered an encounter. Demographic and clinical data from the electronic medical record were recorded for up to 7 days for each ICU encounter that received at least one day of EN. Patients receiving exclusive oral or parenteral nutrition (PN) were excluded. Nutrition goals were determined by the ICU dietitian. EN provided was captured as one of three possible formula groups: standard protein of ≤ to 20% protein calories (SF); high protein of 21-25% calories (HP) and very high protein (37%), low carbohydrate (29%) VHP. Non-nutritional calories from lipid-based medication and dextrose were recorded, in addition to nutrient intake from oral, EN, PN and modular supplements.
Results:
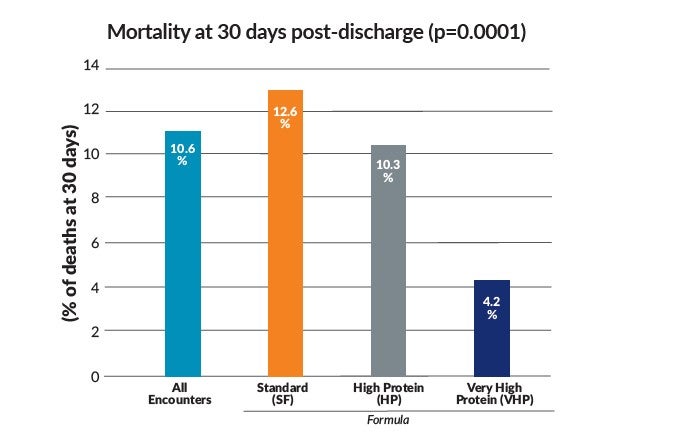
Total of 1,507,858 charts were screened; 3205 met inclusion/ exclusion criteria. The first sequential 2000 encounters were included in the analysis, an estimate to be representative of clinical practice. 1899 mixed medical and surgical ICU patients comprised the 2000 encounters for a total of 12,321 ICU days. Characteristics of VHP formula recipients included 57.5% female, median BMI of 36.8 and more frequent diabetic diagnosis. Sequential Organ Failure Assessment scores were similar across the 3 formula groups. Calorie and protein delivery was measured through ICU-day 7. While all patients received similar calories throughout the measured days, the VHP group achieved a median intake of 103.9 grams (g) protein by day 7 versus 64.3 g in the SF group and 82.3 g in the HP group. Lower amounts of protein were delivered across all 3 groups the first 3 days of ICU stay, with a gradual increase in delivery through day 7. Clinical outcomes showed non-significant differences in hospital length of stay (LOS), inpatient mortality and 30-day readmission among patients discharged alive. ICU LOS was highest in the VHP group by ~0.9 additional days. Ventilator days were higher in the HP and VHP group by one additional day. History of dialysis was higher in the SF and HP groups. Inpatient deaths or deaths within 30 days of discharge and deaths within 30 days of discharge among patients discharged alive was significantly lower in the VHP group, respectively (p=0.0035 and 0.0004).
Discussion:
Catabolism and muscle loss is rampant in the critically ill. Early provision of full calories generally fails to spare muscle or achieve protein anabolism. Multiple randomized controlled trials have failed to show clinical benefit of providing full caloric support in the ICU. Critical care nutrition is currently in a paradigm crisis, forcing clinicians to reassess what and how much nutrition to deliver to patients. A gradual increase in protein over time with a goal of 1.3 g/kg/day by day 7 is suggested by some guidelines. The delivery of higher amounts of protein and lower amounts of calories is particularly challenging with conventional formulas where the calorie to protein ratios risk an excessive delivery of calories while providing limited amounts of protein. In addition, providing lower CHO feedings with high protein delivery improves glycemic/metabolic control. This study demonstrates that providing a VHP, lower CHO formula during the first 7 days of ICU stay is safe and may have a beneficial effect on 30-day mortality. Effect on muscle mass was not studied.
Conclusions:
The gradual increase in delivery of VHP (37% protein and 29% CHO) enteral formula during the first week of ICU stay is safe and conforms to ICU nutrition guidelines, allowing a gradual increase in protein delivery and accumulation of a moderate caloric deficit during the acute phase of critical illness. Future prospective randomized controlled trials are needed to determine maximal clinical benefit of initiating VHP nutrition support in the ICU.
The complete study may be accessed at: https://www.sciencedirect.com/science/article/pii/S0261561422003818
*Past Nestlé Employee **Current Nestlé Employee
Study summary prepared by Nestlé Health Science. All trademarks are owned by Société des Produits Nestlé S.A., Vevey, Switzerland. ©2022 Nestlé Health Science. All rights reserved.